This article is a part of your HHCN+ Membership
The home health industry is once again in line for a major regulatory change. This time, it’s the looming expansion of the Home Health Value-Based Purchasing (HHVBP) Model, which has been active in nine demonstration states since 2016.
As part of its most recent home health proposed payment rule, the U.S. Centers for Medicare & Medicaid Services (CMS) called for a nationwide HHVBP rollout, with the first performance year for most agencies being 2022. Under the likely expansion, agencies will compete on several performance measures against peers across the U.S. for a maximum bonus — or penalty — of 5%.
In this HHCN+ report, Home Health Care News breaks down the mechanisms of HHVBP, assesses the model’s potential upside and summarizes proven success strategies.
Key takeaways from the report:
— HHVBP will propel the home health industry into a new era of value-based care, but true upside and downside risk will be difficult to obtain.
— Providers wondering about ROI shouldn’t only consider bonus payments or penalties. Investing in HHVBP success has several other indirect benefits, including improvements in star ratings and more risk-sharing opportunities with non-Medicare payers.
— While generally supportive of the HHVBP expansion plan, home health experts have several concerns they’re urging CMS to address. Among them: a failure to reward agencies for taking on complex cases where patients are unlikely to improve.
— Home health operators should prepare for HHVBP by investing in data and documentation processes, in addition to clinician education. What’s likely to work in 2022 might change down the road, however, as CMS has a history of fine-tuning its value-based purchasing initiative.
The history of HHVBP
The CMS Innovation Center implemented the HHVBP demonstration effective Jan. 1, 2016. The overarching goal of the program was — and still is — to improve quality and efficiency of care among Medicare-certified home health agencies through financial incentives.
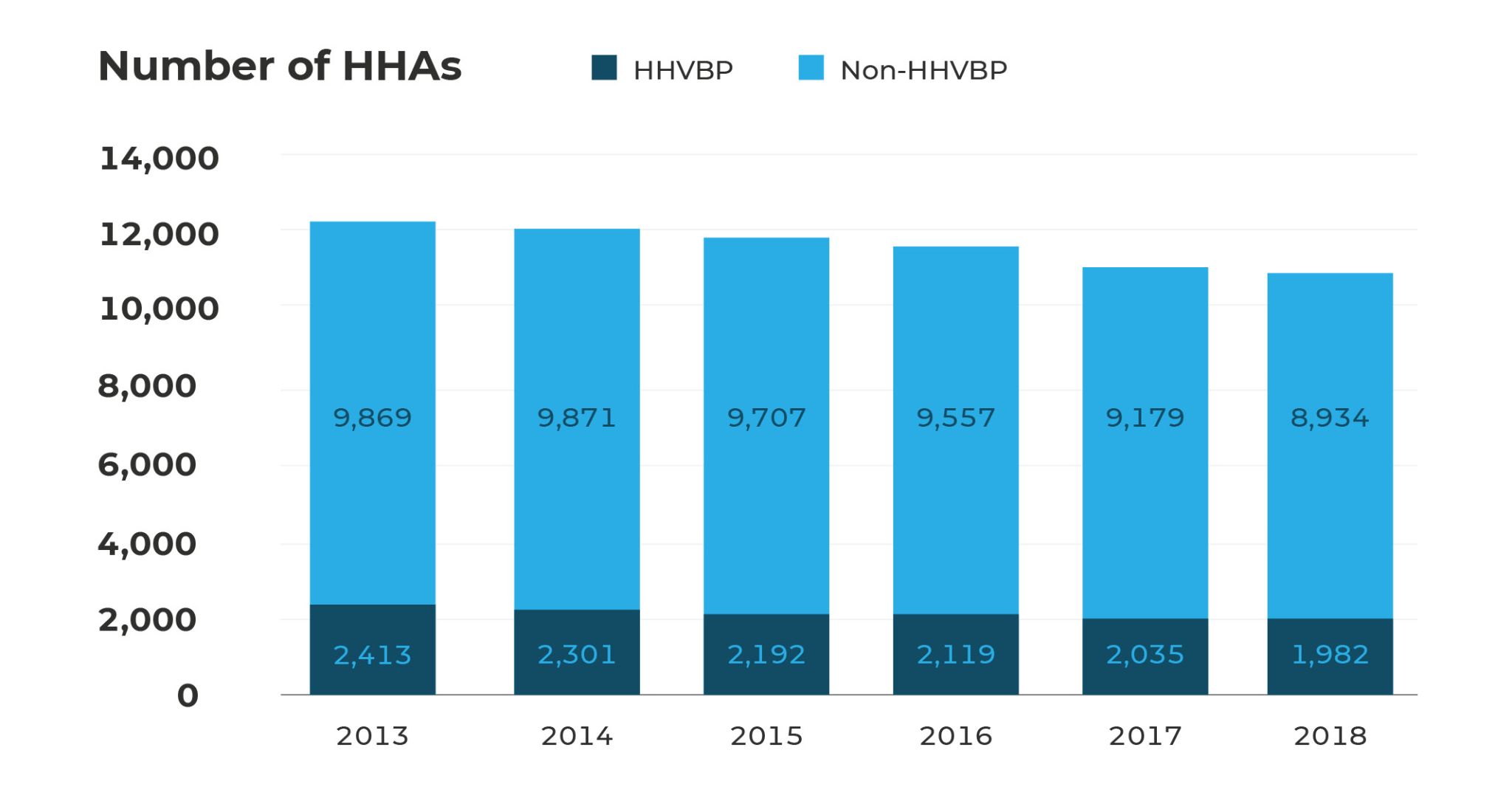
Up until now, agencies in just nine states have participated in the mandatory demo: Massachusetts, Maryland, North Carolina, Florida, Washington, Arizona, Iowa, Nebraska and Tennessee.

When it first launched, HHVBP based its financial incentives on 20 different performance measures, three of which were self-reported. Broadly, those measures were sourced from OASIS items, claims data and HHCAHPS surveys.
In Performance Year 4, CMS tweaked HHVBP’s framework by getting rid of certain measures and adding others, including two new composite measures unique to the demo. Some industry insiders believed the fine-tuning meant that a national expansion would inevitably follow.
“What CMS was trying to do was raise the bar on home health agencies,” Tim Ashe, chief clinical officer at the international software and professional services company WellSky, told Home Health Care News. “And as we raise the bar, we become more efficient in providing home-based care. “We become more effective, with a mindset and an eye toward quality for the individual, as well as satisfaction for that individual.”
Mechanically, CMS used 2015 as the “baseline year” for home health organizations participating in the demo. All following years have been “performance years” grading agencies against their 2015 metrics, with upward or downward payment adjustments officially starting in 2018.
2018 (based on 2016): a maximum payment adjustment of 3%
2019 (based on 2017): a maximum payment adjustment of 5%
2020 (based on 2018): a maximum payment adjustment of 6%
Before CMS unveiled its proposal to expand HHVBP to all 50 states starting next year, the plan was to continue increasing upside and downside adjustments to 7% and 8% in 2021 and 2022, respectively. Additionally, if its proposed rule is finalized as is, CMS would jump over 2020 entirely.
Under the demo, CMS has calculated payment adjustments by assigning home health agencies “points” for both achievement and improvement, then taking the highest of the two to determine an overall “total performance score” (TPS). That TPS figure is then entered into something called a “linear exchange function” that allows CMS to redistribute payments from low-performing agencies to higher performers, with agencies competing against one another on a state level.

How have agencies in the nine demo states performed thus far? Pretty well, it turns out.
“If you read the CMS data, they say that those nine states have done very, very well,” DeAnn Briscoe, senior director of clinical education at home health coding and consulting firm MAC Legacy, told HHCN. “They increased their quality by 4.6%. They saved Medicare an average of $141 million annually.”
CMS, in fact, has repeatedly cited HHVBP as one of the CMS Innovation Center’s most successful initiatives ever.

Since its 2010 launch, the center has rolled out 54 alternative payment models that compensate health care providers for delivering high-quality care while lowering costs.
Of these, just a handful — including HHVBP — have accomplished that mission.
“[HHVBP] is a great example of how the Innovation Center can design successful models that both improve quality for Medicare beneficiaries and lower costs,” Brad Smith, the center’s former leader, said in January 2021. “Over the past year, we have taken a data-driven approach to assessing all the Innovation Center’s models, and we are excited that HHVBP has met our gold standard for expansion as laid out by Congress.”
Washington, D.C.-based research and consulting firm The Moran Company has estimated that a 50-state HHVBP program would result in about $6.3 billion in savings over a 10-year period, using Congressional Budget Office (CBO) scoring methodology.
In 2018, the payment adjustment in HHVBP ranged from a 1.5% penalty for providers in the lowest-10th percentile to a 1.5% bonus for providers in the highest-10th percentile, according to an investment note from Bank of America. CMS previously stated that the average adjustment was a 0.85% bump in 2018.
Slideshow: HHVBP payment adjustments by agency type



The bar charts in the slideshow above show the payment adjustments that different types of home health agencies received in calendar year 2020. Click the left or right arrows to change slides.
The CMS expansion plan
As part of its HHVBP expansion plan for 2022, CMS is proposing to keep many aspects of the current demonstration the same, at least from a big-picture perspective. Yet the agency is floating several major changes to the model as well, some of which home health providers are firmly against.
Here are a few of the biggest:
Key difference #1: Instead of 2015, 2019 will be used as HHVBP’s baseline year, with 2022 being the first performance year and 2024 being the first payment year. The baseline year for new agencies will be their first full year of services beginning after the date of Medicare certification. Agencies certified in 2019 will use 2021 as their baseline line due to the COVID-19 pandemic.
Key difference #2: Instead of progressive incentives potentially topping out at 8%, agencies will be exposed to a 5% upward or downward payment adjustment in all HHVBP years.
Key difference #3: The demo compares home health agencies to in-state peers, meaning an agency in Florida is only compared against other Florida providers. As part of its expansion plan, CMS is proposing to have home health agencies compete on a national level, meaning home health agencies in Florida will be weighed against home health agencies in New York, for example.
Key difference #4: Agencies will also compete against organizations that are similarly sized, with CMS categorizing operators into “small” and “large” cohorts based on beneficiary count in the prior calendar year. Just under 7,100 agencies will fall within the larger-volume cohort, with 485 agencies falling within the smaller-volume cohort, according to MAC Legacy data.
If its proposal is finalized, CMS will calculate HHVBP payment adjustments using a process that’s similar to the demo. Claims-based measures will account for 35% of a home health agency’s overall score, with OASIS-based measures also accounting for 35%. HHCAHPS measures will account for 30% of an agency’s score.
Those percentages will be weighted differently if an agency is missing a measure category or specific measure.
“This is a positive move,” Ashe said of the expansion plan. “It’s establishing clarity around the value of home health and potentially other home- and community-based services as a part of a formal solution to improve quality and lower health care costs. So I’m really bullish on this.”
Analyzing ROI
Located in Kirkland, Washington, and part of a broader health system, EvergreenHealth Home Care is one of the largest home health and hospice providers in the Pacific Northwest. The organization handles roughly 11,000 home health and hospice episodes of care each year.
Thanks to investments around clinician education and information integrity, it has been among Washington’s top HHVBP performers since 2016.
“We have done better as the years have gone by,” Molly McDonald, the clinical quality coordinator for EvergreenHealth’s home health and hospice business, told HHCN. “There were a few quarters where we maybe took a few steps back, if you look at the percentiles and things like that. But overall, we continue to progress every year.”
EvergreenHealth Home Care wasn’t always known for its quality. In 2015, it only had 2.5 stars.
Knowing it had to turn its operations around to avoid HHVBP penalties, EvergreenHealth Home Care invested heavily in its data and documentation processes, turning to BlackTree Healthcare Consulting as one of its consultant partners.
“If you don’t have a data vendor, get one,” McDonald said. “They should be your best friend.”
The provider also doubled down on clinician education, ensuring that its staff members were all OASIS experts and training in patient-centric care.
Part of that additionally included the formation of dedicated workgroups around targeted HHVBP performance metrics.
“Build an army of experts who are actually doing the work,” Brent Korte, the chief home care officer for EvergreenHealth, told HHCN. “Have your clinicians be front and center. Make sure they know the answer to, ‘What is HHVBP’? Make sure they know, ‘How does my charting, how does my clinical care relate to the success of our agency?’”
As a result of those and other investments, EvergreenHealth turned into a 4- or 4.5-star home health provider in all following years.
“This was a cultural change within our operation,” Korte added. “We sort of use it as a great way to further engage our clinical staff. They are competitive. They want it to succeed, and they love knowing that they’re part of an organization that is doing well.”
From an ROI perspective, EvergreenHealth’s HHVBP investments paid off in the form of star-rating improvements and staff-satisfaction gains. While those are certainly positives, Korte and his team were anticipating greater upward payment adjustments compared to what EvergreenHealth actually received.
“Our simple strategy was this: Let’s have the best outcomes and get paid. It’s kind of a no-brainer, right?,” Korte said. “But the actual payment was significantly less. For the 2018 performance year, the potential upside was 6%. However, we actually got 1.4% — despite being in the top-90th percentile.”
That was one of the most important lessons learned: that HHVBP’s maximum payment adjustments are difficult to reach.
“If you look at Evergreen’s Medicare billables, let’s just assume we’re at around $20 million in straight Medicare,” Korte continued. “We’re talking about upside that would have been $1.6 million. That’s awesome. That would have been something else, but it didn’t translate like that.”
Home health agencies going into HHVBP for the first time should keep that in mind, as a few percentage points can possibly translate into hundreds of thousands of dollars.
“It’s hard to say that we had a net financial gain,” Korte said. “What was the gain? It’s that we built so many more relationships because our star ratings improved. Star-rating improvement is correlated to value-based purchasing success, for sure.”
Looking ahead, Korte said he’s somewhat concerned about the decision to start all home health providers at 2019. For EvergreenHealth, that effectively means all of the HHVBP progress that it’s made since 2015 counts against its performance.
Korte — and several other home health leaders — are also concerned about a perceived failure to account for patient populations with little chance of improvement. In some ways, they argue, HHVBP rewards providers for returning patients to their healthy baseline — not keeping them in the base shape possible as a complex condition worsens.
“The [HHVBP] model needs to recognize that some home health agencies simply care for much sicker and more complex populations than others,” Dan Savitt, CEO of the Visiting Nurse Service of New York (VNSNY), told HHCN during a recent TALKS appearance. “That should be a factor in the risk adjustment models, so agencies can compare fairly and ensure that incentives are aligned to care for patients with complex health and social determinant needs.”
Companies featured in this article:
CMS, CMS Innovation Center, EvergreenHealth Home Care, Mac Legacy, VNSNY, WellSky
